
 Discussion
Discussion
Cold agglutinin disease overview
Last updated Sept. 30, 2025, by Marisa Wexler, MS
 Fact-checked by Marta Figueiredo, PhD
Fact-checked by Marta Figueiredo, PhD
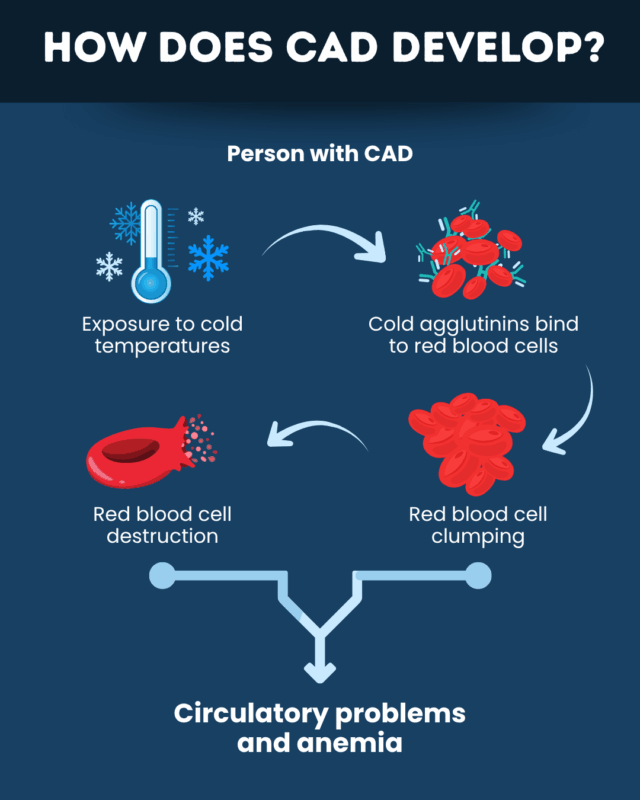
Cold agglutinin disease (CAD) is a rare autoimmune blood disorder in which cold temperatures trigger the body’s immune system to mistakenly attack red blood cells. This leads to cold-induced circulatory problems and anemia (low red blood cell counts) that give rise to CAD symptoms.
Affecting approximately 1 of every 1 million people worldwide, CAD is a rare form of autoimmune hemolytic anemia, a group of conditions in which the immune system attacks and destroys healthy red blood cells.
This blood disorder can have a substantial impact on quality of life, and some CAD complications can be life-threatening. However, treatments are available to manage the disease and prevent complications.
Causes and risk factors
CAD is caused by self-reactive antibodies, called cold agglutinins, that bind to red blood cells at cold temperatures and cause them to agglutinate, or stick together. This recruits proteins from a part of the immune system called the complement cascade, ultimately leading to red blood cell destruction, a process known as hemolysis. The aggregation, or clumping, and destruction of red blood cells lead to circulatory problems and anemia that cause the disease’s symptoms.
While CAD can affect anyone, it is more common among:
- adults, typically manifesting between the ages of 40 and 80
- women, who are twice as affected as men
- people with certain underlying conditions, including some types of infections and cancer
- individuals in cold parts of the world, likely because people living in cooler climates are more likely to experience noticeable symptoms
Types of cold agglutinin disease
There are two types of CAD — primary and secondary — based on whether the disease occurs together with or independently of other health conditions.
Primary CAD occurs in the absence of an underlying condition. It is thought to be the result of an abnormal but noncancerous growth of cold agglutinin-producing B-cells, which are the immune cells responsible for making antibodies.
By contrast, secondary CAD develops as a complication of an underlying health problem, which can be an infection, cancer, or an autoimmune disorder.
While both types can cause similar symptoms and day-to-day management strategies may be comparable, a key difference is that secondary CAD usually requires addressing the underlying disorder to be resolved. As such, it’s important to distinguish between the two forms of the condition to allow for optimal management.
Common symptoms
The nature and severity of the symptoms of CAD can vary greatly between individuals. Commonly reported symptoms include:
- fatigue
- weakness
- dizziness
- shortness of breath
- pale skin
- a rapid heartbeat
Additionally, red blood cell clumping in cold conditions frequently causes circulatory problems. Two main ones are:
- Raynaud’s phenomenon, in which extremities become painful and take on a white or blue color
- acrocyanosis, or a painless blue discoloration of the extremities
A characteristic feature of CAD is cold sensitivity; in other words, symptoms are usually triggered or worsened by cold temperatures. Other potential triggers include infections, major trauma, and major surgeries.
More serious symptoms and signs of CAD include:
- decreased alertness and confusion
- temporary loss of consciousness
- chest pain
- problems with heart rate and blood pressure
- ulcers on the fingertips
CAD also appears to be associated with an increased risk of thrombotic events, which occur when a blood clot blocks blood flow and causes complications.
How CAD is diagnosed
A diagnosis of CAD usually begins with a clinician collecting a detailed medical history and conducting a physical exam. The examination aims to determine if the person is experiencing signs and symptoms indicative of the condition.
Initial blood tests may measure red blood cell counts and levels of hemolysis markers to assess the presence of anemia and hemolysis, two CAD hallmarks. Confirmatory testing includes:
- a direct Coombs test, which detects certain antibodies and complement proteins bound to red blood cells
- cold agglutinin titer testing, which can measure titers, or levels, of cold agglutinins in blood
If a person has complement proteins attached to red blood cells and high cold agglutinin levels, a CAD diagnosis can generally be confirmed. If the type of CAD is unclear, additional tests — such as screening for infections and imaging scans for cancer — should be carried out to determine the type and guide treatment.
Treatment of CAD
Treatment of CAD focuses on managing disease symptoms and addressing any underlying health problems. CAD treatment options commonly include:
- lifestyle changes, such as wearing warm clothes and avoiding cold foods
- medications targeting the underlying disease
- supportive medical treatments to manage symptoms, such as blood transfusions to ease anemia, and special precautions taken when undergoing surgery
Not everyone with CAD will require medical treatment; some people with mild disease are able to get by with lifestyle adjustments alone. Generally, treatment is recommended for people experiencing problematic symptoms that are impacting day-to-day life in spite of lifestyle changes.
When medical intervention is necessary, the type of treatment will depend on the type of CAD.
- In primary CAD, treatment focuses on dampening the autoimmune attack that drives the disease. This typically involves medications that deplete B-cells, such as rituximab, and/or medicines that block complement activation, such as Enjaymo (sutimlimab-jome).
- In secondary CAD, treatment focuses on managing symptoms while the underlying health condition is addressed. Antibiotics may be used to treat bacterial infections, while chemotherapy is commonly used for cancer, and immunosuppressive therapies for autoimmune diseases. Treating the underlying disorder usually leads to CAD resolution.
Regular patient monitoring is essential to track disease activity and assess the response to treatment.
Prognosis and outlook
With treatment, it is often possible to induce CAD remission — when a patient is not experiencing any troublesome symptoms. Many people with primary CAD can stay in remission for years, and some may even be cured.
For people with secondary CAD, the prognosis is usually defined more by the severity of the underlying condition than by CAD itself. For example, bacterial infections can often be cleared up quickly with antibiotics, whereas treatment of cancer may be more arduous and uncertain.
CAD can have a substantial impact on patients’ quality of life, especially when symptoms flare up due to cold temperatures or other triggers. Although fatal complications of CAD are rare, some studies have indicated that people with CAD have a higher risk of death, especially during winter.
Living with CAD
Living with CAD often requires patients to make changes in their day-to-day routines to help manage the disease.
Some practical tips for navigating life with CAD include:
- staying in warm places where possible
- wearing warm clothing
- avoiding cold food and drinks
- wearing gloves when getting things out of a refrigerator
- using heaters as needed
- minimizing the use of air conditioning
- getting recommended vaccines and regularly washing hands to avoid infection
Living with CAD can be challenging, but no one needs to do it alone. Organizations such as the Cold Agglutinin Disease Foundation, the National Organization for Rare Diseases, and the Autoimmune Association offer resources that may be useful for CAD patient support.
Cold Agglutinin Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
 Discussion
Discussion
-
Discussion
-
 Discussion
Discussion
-
Discussion
-
 Discussion
Discussion